Hair transplant is a relatively new and continuously evolving art, which has seen several advances, paving the way for more natural results for patients. As with any other surgical procedure, complications may occur, and these present a major challenge for the surgeon and the patient. With increasing popularity, the number of surgeries continues to rise. More importantly, as the technique becomes popular, doctors from different specialties, often with inadequate training, have performed the surgery, and consequently, the total number of complications has shown an increase. A complication is an adverse event that is not considered to be a common or usual occurrence and which requires a change in methodology. Hair transplantation is a cosmetic surgery, and hence, any complication can seriously impact the cosmetic and psychological outcome for the patient and can have medicolegal implications. Hence, the surgeon and the staff should be familiar with all possible complications, techniques for prevention, and also techniques for their management.
The following are the general surgical complications that occur during hair transplantation:
Anesthesia: The overwhelming majority of adverse reactions to local analgesics are psychogenic in nature and related to fear. True immunologic reaction to a local anesthetic is rare. Irrespective of the fact that a patient has received local anesthesia in the past, we advocate sensitivity testing for all.
Intraoperative complications: Tachycardia can occur when tumescent fluid containing adrenaline is given. This is usually transient. However, in a patient with cardiac compromise, this may pose a risk. Hence in all patients, particularly those above 40 years of age, an electrocardiogram and physician assessment for anesthesia fitness are indicated. It is also recommended to monitor heart rate and blood pressure levels throughout the procedure, especially during anesthesia administration.
Postoperative complications: Syncope is a complication, which often occurs at the end of surgery, particularly if it is a long surgery. This may be due to pain, postural hypotension, poor hydration, hypoglycemia, and so on. Proper anesthetic and analgesic precautions and minimizing Xylocaine usage by completing the surgery as quickly as possible are advised. Maintaining hydration and electrolyte balance during surgery, avoidance of sudden change in posture may help in reducing the chances of syncope.
Pain during and after surgery is a common complication and is easily handled by proper surgical technique and use of analgesics. Factors that contribute to pain include wide strip, bleeding, wound tension, and large sessions with inadequate anesthesia. In addition, ice packs and vibrators can also be used to minimize the pain during anesthetic injection (vibrasthesia). Adequate postoperative analgesia can be achieved by nonsteroidal anti-inflammatory drugs and other analgesics.
Postoperative edema can occur over recipient area. Oral steroids in postoperative period can be used to reduce it.
Postoperative itching is common on donor as well as recipient area. Drying and crusting can be the reason. Saline spray for 3–4 days for multiple times can reduce itching. Head wash may help in effective control of itching.
Infection: Localized infections can occur in both recipient and donor areas. The incidence of low and serious infections is rare (<1%), which may be due to poor hygiene, excessive crust formation, or a preexisting medical risk factor. A high-tension closure at the donor site leading to circulatory compromise and pronounced crust formation can increase the risk of infection. Recipient-site infections often present with papulo-pustules localized to the affected area.
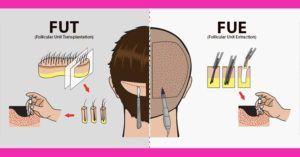
Complications after FUT Hair transplant procedure
Donor-site wound dehiscence is extremely uncommon because higher vascularity of scalp favors faster healing of incisions. However, circulatory compromise occurring because of factors such as diabetes, a high-tension closure, coexisting suture line infection, premature removal of sutures, and excessive early physical activity places the patient at a greater risk for unexpected donor-site dehiscence.
Necrosis and wound dehiscence: Wound dehiscence, a rare phenomenon, is a sign of delayed healing or nonhealing. Necrosis of the wound margin is a result of ischemia. A technical error during closure creating excessive tension along the incision line can produce localized microcirculatory collapse resulting in necrosis. It is a serious complication because the soft tissue gets destroyed, and in the process, the follicles within the area get permanently damaged.
Caution is advised while closure to avoid excessive tension along incision line, especially near the area superior to the mastoid process, and in wide strips done for mega sessions. Avoiding any forced wound closure and using a multilayered closure to approximate only those areas along the incision line with favorable tension dynamics are advised.
Donor hair effluvium: Commonly referred as donor shock loss, it can be seen above and below the line of incision but is usually temporary, and full recovery is almost always seen in the following 3–4 months. Surgical consequences such as alteration of natural follicular population, edema, inflammation, and suture line vascular compromise are probable causes. A dramatic hair loss may be seen in accidental major vascular damage. Local wound care with daily cleaning and topical antibiotics along with measures to control post-op inflammation has been advocated.
Scarring: Wide scar, though uncommon, is a possibility as a result of faulty surgical technique or poor patient compliance. Scar maturation takes weeks or even months, which leaves the wound strength vulnerable to patient activities after suture removal. Neck flexion restrictions if not followed may increase donor-site tension resulting in wide scars. Visible scarring is the most common issue and can be seen due to multiple factors.
Causes of visible scarring include the following:
- Use of multiple donor incision lines scattered throughout the donor region.
- Strip excisions that are placed in the inferior donor region where the prevalence of scar stretching is increased.
- When strip harvests venture superiorly into donor-site fringe zones that possess a risk for future thinning.
- Visible scarring is one complication that brings the strip dissection to disrepute as young men have a tendency for changing their hair styles, and with short hair, the scar becomes visible. Hence, this needs to be avoided at all cost.
Keloid and hypertrophic scars: Keloid or hypertrophic scar is a rare entity and occurs because of exaggerated response to healing. In hypertrophic scar, normal surrounding skin is not involved as seen in keloid. Local steroid ointment application or steroid injection is needed. Keloid involves normal surrounding skin. Most of the time, patient complains of itching, pain, and sometimes pricking sensation over keloid. Intralesional steroid injections control sign, symptoms and growth of the keloid. Keloids are uncommon and can be avoided by careful patient selection.
Neuralgias, neuromas, and hypesthesia: Careless deep incisions can cause transection of the greater occipital, lesser occipital, or auriculotemporal nerves, resulting in hypesthesia localized to the innervation zone. Aberrant neural healing can cause persistent scalp hyperesthesia or regional discomfort. Regional infiltrations of local anesthetics and corticosteroids intralesionally can be used to treat neuropathic pain or hypersensitivity arising from an injured nerve.
Hematoma: Though rare, deep incisions can lead to donor-site hematomas because of a major artery transection. Limiting donor-site incision depth and carefully exploring the wound bed for the evidence of vascular damage can avoid this complication. Major vessel transections require careful suture ligation for effective control. A multilayered closure technique is preferred to eliminate any dead space that could potentially harbor a fluid collection.
Complications after FUE Hair Transplant
Minimal invasion during surgery ensures less frequent complications after FUE. Nevertheless, many complications have been reported, which are as follows:
Donor-site depletion: Irrespective of whether scoring was performed by manual, motorized, or robotic punches, the risk of a clinically apparent depletion of hair from the donor region because of aggressive and nonuniform harvesting is observed. This may create an iatrogenic “moth-eaten” or “pseudo-syphilitic” appearance
Pinpoint scaring: It is a misconception that FUE is a scarproof technique. The punch used to harvest each follicular grouping may create pinpoint white atrophic macules. In the hands of a skilled surgeon, most of them are not visible to the human eye, and even if visible, they are far less noticeable than a linear scar of FUT for most patients. Nevertheless, patients should be informed about the possibility that these pinpoint white scars or hypopigmented macules may be visible on close inspection with short hair.
Postoperative effluvium: A possibility of postoperative donor hair effluvium is reported, which can happen post-surgery. The condition may appear after few days to few weeks of the surgery and show diffuse hair loss. It is mostly temporary and resolves within 3–4 months in most of the cases. The most common cause can be overharvesting and/or hampered blood supply.
Buried grafts: They can be seen most commonly when blunt punches are used. If punching is performed in hurry or proper alignment of punch along with hair follicles is not carried out, then the graft is pushed into the dermis leading to buried graft.
Overharvesting: It may lead to permanent damage of the donor area, thinning, and patchy hair loss. Before starting the extraction process, safe donor area should be demarcated and overharvesting should be avoided. Hence, it is preferable not to exceed extraction of more than 1:4 follicular units.
Necrosis: Cutaneous necrosis after FUE is very rare.
Subdermal cysts: They present as multiple, slow-growing nodular, painless swellings in the scalp donor area. Lack of due diligence while performing FUE can lead to subluxation of the grafts into the subdermal layer of scalp. Over tumescence of the scalp donor area, use of blunt punches, and trying to “core” out the full-thickness grafts can all contribute to this. Hence, it is advisable to remove all grafts from the donor area.
Keloid: A thorough search of literature found two case reports of keloid or hypertrophic scar formation at donor site following FUE.
Other rare complications: Lichen planopilaris has been reported after FUE as well as strip method possibly because of the precipitation of autoimmune reaction of transacted hairs. Alopecia areata is another rare complication. Trichorrhexis nodosa too has been reported.
Recipient Area Complications
Chronic folliculitis, though uncommon, can be seen as a result of failure to maintain hygiene or because of some preexisting dermatological disorder. This is usually a foreign body reaction to poorly dissected hairs- damaged shafts – Pus is sterile. Aggressive treatment with topical and systemic antibiotics and daily cleansing with antibacterial shampoo are advocated to prevent cicatricial scarring.
Cysts appear as small skin-colored swellings around the transplanted hair follicles, which can become erythematous and painful. They result because of small grafts slipping under the skin or from piggybacking one graft on top of the other. Treatment consists of incising the cysts and expressing out the contents, using warm compresses, or sometimes applying topical antibiotics.
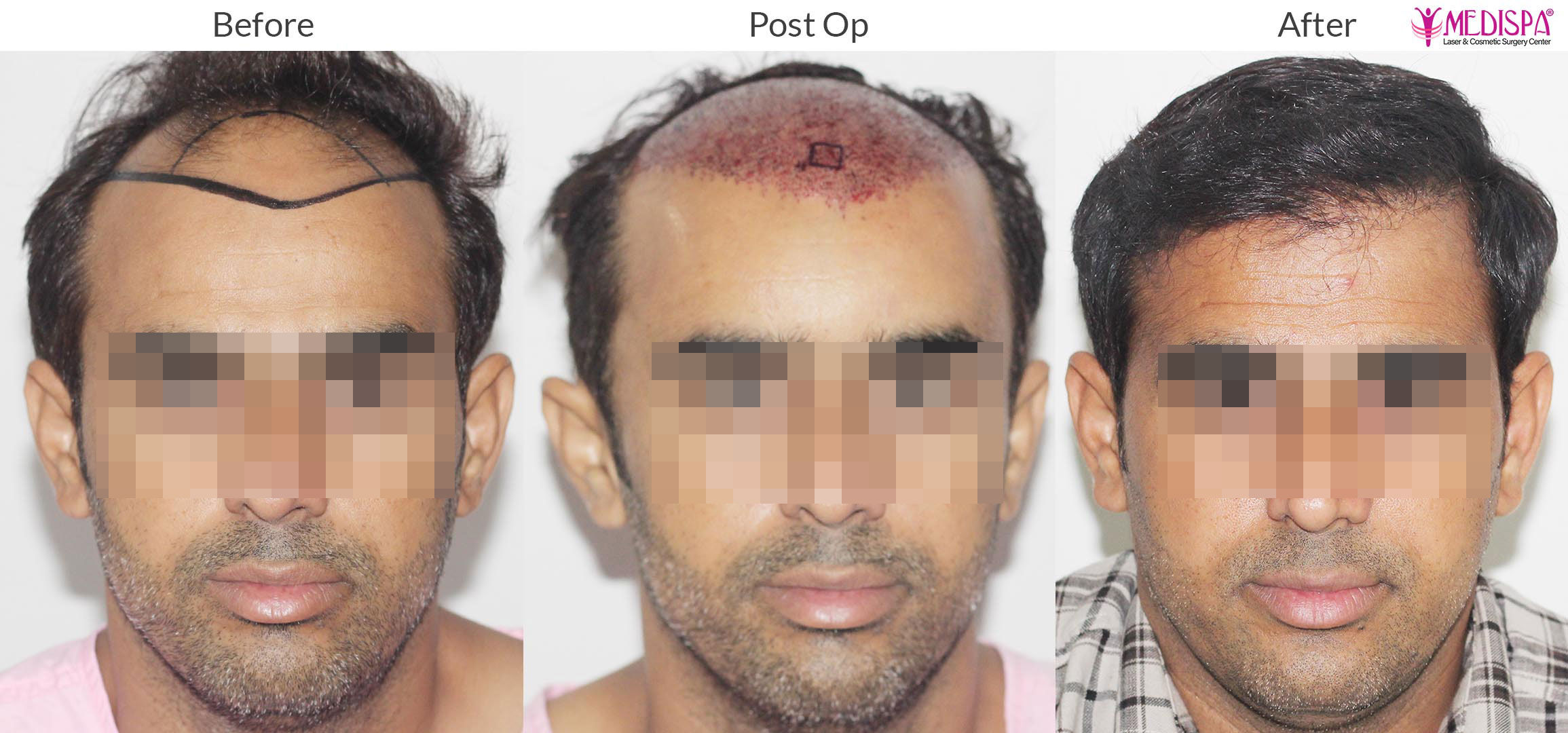
Unnatural/poor hairline: The surgeon should be very cautious in designing and surgical technique; hairline is the surgeon’s signature. Unnatural appearance of transplanted hair is a complication of a poor design and surgical execution.
Low-positioned hairline and blunting of the temporal angles can occur if placement is below 6cm from the glabella. It creates artificial appearance in cases with higher grades of baldness or global thinning. It can also lead to dissatisfaction of the patient over time, especially in the case of evolving progressive hair loss behind the transplanted hairline. Creating zones of variable density in a patient with a Norwood V pattern to mimic the distribution pattern of hair in someone who is a Norwood III gives a very natural result.
Improper angulation of the hair grafts is also a common complication. Follicular single unit or multiunit transplantation is the gold standard in hair restoration surgery (HRS), but the right angle and the direction of the transplanted hair are critical to the outcome and naturalness following HRS, especially in the hairline and frontal areas.
Conclusion:
Henceforth, the rate of complications involved in hair transplant surgery is very rare if a highly experienced hair transplant surgeon is selected for your procedure. The complications are seen in individuals who fall in trap of a unskilled and inexperienced surgeons who are not even qualified to perform the hair transplant surgery. So it is our highest recommendations to select your hair transplant surgeon carefully after researching extensively on the success rate and surgical skill of the hair transplant surgeon.